 Life & Style
Life & Style

Hot weather affects durian crops in Bà Rịa - Vũng Tàu Province.
1.
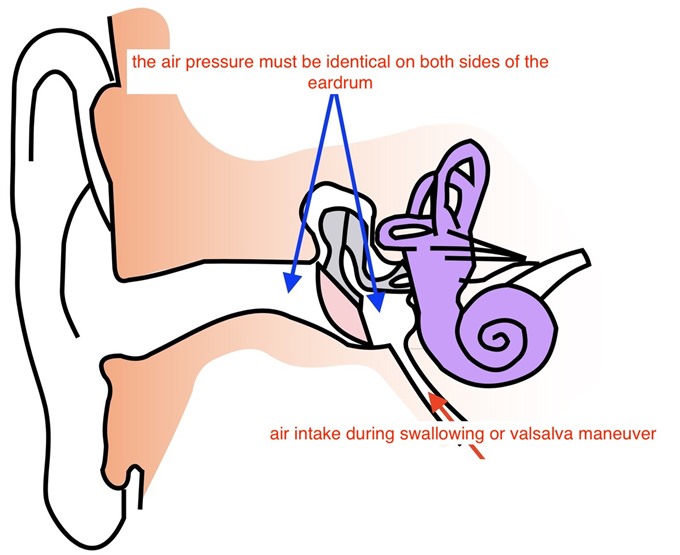
OME is a chronic collection of non-infected fluid in the middle ear. The middle ear is an air cavity closed to the outside by the eardrum and ventilated through the eustachian tube connecting the ear to the upper part of the back of the throat, which leads up into the nose.
 |
| Dr. Dominique Garcia — Photo courtesy of Hanoi French Hospital |
By Dr. Dominique Garcia*
What is otitis media with effusion (OME)?
 |
OME is a chronic collection of non-infected fluid in the middle ear. The middle ear is an air cavity closed to the outside by the eardrum and ventilated through the eustachian tube connecting the ear to the upper part of the back of the throat, which leads up into the nose. The tube helps to equalise the pressure between the air around you and the middle ear, and to drain fluids. If it gets blocked, fluids cannot drain and may accumulate behind the eardrum.
OME is more common in children between 6 months and 3 years old but can also occur in younger schoolchildren. It usually resolves itself within 1 to 2 months. However, especially with a long cold season as in Hanoi, fluid may persist for longer and cause temporary hearing impairment. Signs and symptoms are neither acute nor dramatic, and OME is often overlooked.
 |
What causes OME?
There are several reasons why the eustachian tube may block:
Any child can develop OME, but there is increased risk for those with
Signs and symptoms?
These may vary but the most common are
Please remember that most commonly, the symptoms are very mild. Always make sure you see your child’s doctor for an accurate diagnosis and to discuss what should be done for your child if you are concerned that something may not be quite right.
Diagnosis and treatment?
Your doctor will review your child’s medical history and perform a physical examination, part of which is the inspection of the eardrums. The doctor uses an otoscope to look inside the ear and to blow air into the ear canal to check the eardrum’s movements. This examination is pain-free. He may order additional tests to rule out infection or hearing loss.
 |
| T ventilation tube. — Photo courtesy of Hanoi French Hospital |
Treatment can vary from child to child, and your pediatrician will discuss with you the most appropriate treatment for your child. Most OMEs resolve within six weeks and do not require any treatment.
Treatment with steroids, antibiotics, decongestants or antihistamines is not recommended, because their long-term effectiveness is uncertain and they may cause significant side effects and risks.
Auto-inflation has been shown to be the only beneficial, low-risk and low-cost non-surgical therapy but equally has limited effectiveness.
Ear tubes
If your child has OME lasting more than 4 months and has frequent ear infections or hearing loss that may affect his learning abilities, your child’s doctor may suggest the insertion of tympanostomy ventilation tubes to be placed in the eardrums. This form of treatment is currently the only one to promote healing, at least for the duration of the tube’s placement.
 |
| Coil ventilation tube. — Photo courtesy of Hanoi French Hospital |
The principle is to make a small opening in the eardrum (paracentesis or myringotomy) and prevent it from closing by inserting a small ventilation coil, or T tube, to drain the fluid and relieve the pressure from the middle ear, allowing air to enter. The procedure is pain-free and performed in day-care, under general anesthesia to make it as comfortable as possible. Usually your child can return home after 3-4 hours. Hearing is restored after the fluid has drained, almost immediately. There are two types of tubes that commonly fall out on their own after 8 to 18 months. Most children with OME recover quickly. However, in up to 20% of those under 7 years old, OME can reoccur, requiring repeat intervention.
If your child had ear tubes inserted, monitoring is important to ensure proper recovery and water, especially soapy bath water, should not be allowed to penetrate the ear.
If you have any questions or concerns about your child’s condition, please talk to your pediatrician or ENT specialist.
Ref : F. Simon et al., International consensus (ICON) on management of otitis media with effusion in children; Eur Ann Otorhinolaryngol Head Neck Dis. 2018 Feb ;135(1S : S33-S39).
* Dr. Dominique Garcia is a visiting ENT and Head & Neck surgeon from France. He is part of Prof. Pierre Verdalle’s team of highly qualified French doctors who continually provide their expertise and know-how to the Hanoi French Hospital and its patients.
If you have any questions or concerns regarding your child’s health, please contact us at 84 – 24.3577.1100, access www.hfh.com.vn, or email us at contact@hfh.com.vn. Address: 1 Phương Mai, Đống Đa, Hà Nội.
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
Something colourful, something weird, something scary: This is how visitors often choose to describe the 13 beautifully decorated masks from the Torres Strait on display in the exhibition “Evolution: Torres Strait Masks”, which introduces the masks in digital format and opened on Friday at the Việt Nam Museum of Ethnology in Hà Nội.
 Life & Style
Life & Style
The Agri-Tourism (Agriculture in combination with Tourism) has seen as potential in Việt Nam, but the new service has yet took off with a lack of standard criteria and linkage among locals as well as strategy plan in human resources training and promotion.
 Life & Style
Life & Style
A work of art depicting highlights of the
 Life & Style
Life & Style
A father lifts up his son in Hến Dune in the central province of Thừa Thiên-Huế. — VNS Photo Việt Thanh
 Life & Style
Life & Style
Trần Đức Huy, a student of the physics specialised class of Hanoi-Amsterdam Gifted High School, brings pride to Việt Nam when he received the award for the best contestant of the host country and a gold medal in the 19th Asian Physics Olympiad organised in Việt Nam early this month.
 Life & Style
Life & Style
Anyone visiting an island in the East Sea of Việt Nam may be impressed by the vegetable gardens grown by soldiers. All kinds of containers are used to store soil brought from the mainland to raise vegetables.
 Life & Style
Life & Style
Talented composer Nguyễn Văn Chung and dozens of young singers will perform in a free concert at HCM City’s Bến Thành Theatre for children on Sunday.
 Life & Style
Life & Style
The large-scale event, organised by the Việt Nam Fine Arts Association, yesterday attracted 500 art works by 60 professional logo designers from across the country.
 Life & Style
Life & Style
Photo of the Day - Peak season












